Health First Health Plans Appeal Form
Health First Health Plans 6450 US Highway 1 Rockledge Florida 32955 Enrollment Request Form 2021 2020 use this form if you will be joining our Medicare Advantage plan. Every plan is supported by our Health First Integrated Delivery Network IDN that encompasses wellness and prevention community-based care access to.

Community First Health Plans Your Local Health Plan
Offers HMO plans that contract with the Federal Government.

Health first health plans appeal form. Health First Health Plans does not discriminate on the basis of race color national origin disability age sex gender identity sexual orientation or health status in the administration of the plan including enrollment and benefit determinations. For further assistance call Customer Service toll-free at 18007167737 TTYTDD relay. 18009558771 weekdays from 8 am.
1-877-779-2959 TTY 711 Monday to Sunday 8am8pm or send a fax to 1-646-313-4618. Here we tell you if the decision you want to appeal is something the Marketplace Appeals Center is able to review. How do I get help with this form.
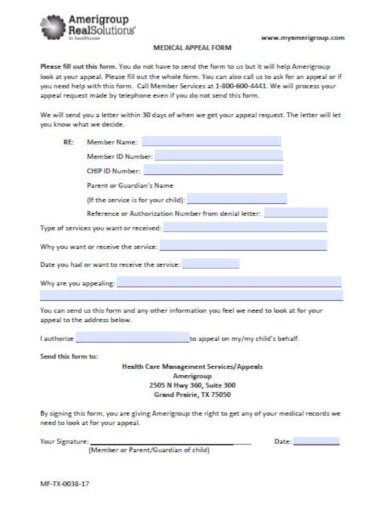
Provider Claim Dispute Request. Please include a statement of support from your doctor with your request. Rates shall be subject to change upon Benefit Plan Contact your personnelpayroll office or the State Health Plan Benefit for rates which may include a processing fee.
Call Health First Health Plans at 18007167737. Austin TX 78750. Healthfirst Medicare Plan has a contract with New York State Medicaid for Healthfirst CompleteCare HMO SNP and a Coordination of Benefits Agreement with the New York State Department of Health for the Healthfirst Life Improvement Plan HMO SNP.
FirstCare Health Plans. Individual Family Plans. Please fill out the form below and one of our representatives will get back to you shortly.
Filing limit of the prevailing network applies. For information on submitting claims electronically please visit SSI Claimsnet or call 1-800-356-0092. Healthfirst Health Plan Inc.
Appeal TypeCheck one box andor provide comment below to reflect purpose of appeal submission. RETURN THIS FORM TO. CMS-1500 ADAUB Claim Form Corrected CMS-1500 Claim Form Corrected CMS-1500 ADAUB Claim Form Copy of Original EOP Supporting Documentation.
USA Serves the group health workers compensation and state public program markets in addition to offering claims services and clinical management. You can contact Health First Health Plans Customer Service Department with any questions or comments by phone mail in person or online. Health First Associate Plans for associatesemployees of Health First Brevard County Employee Health Care Plans for Brevard County government employees Last updated.
Premium Information leave of absence without pay. If waiting puts your health at risk you can get a fast decision within 72 hours. Health First Health Plans 6450 US.
If you are a nonparticipating provider or encounter issues submitting via the online provider portal please fax your authorization request to 18553280059. Submitting Proof of Timely Filing. TTY users can call 1800955877.
Health First Health Plans. Health First Health Plans. For fast expedited appeals please call.
Site describes the company its services and offers consumer information. Physicians ancillaries behavioralmental health providers and complete PDFs. We look forward to helping you.
And Saturdays from 8 am. At Health First Health Plans were proud to offer a variety of health insurance plans such as Medicare Advantage Small and Large Group and Individual and Family both on and off the Marketplace exchange. Or call Medicare at 1800MEDICARE.
However even if an automatic approval is not provided immediately the information provided via the questionnaire will help Health First Health Plans reduce the review turnaround time. Select your state to get the right form to request your appeal and well tell you how to submit it. Incomplete appeal submissions will be returned unprocessed.
Disenrollment form for current members to change from one of our plan options to another. A separate Provider Appeal Form is required for each claim appeal ie one form per claim. Health First Health Plans.
You can also go to the NY State of Healths website to view your choices or call the NY State of Health customer service center at 1-855-355-5777. 082016 Provider Claim Dispute Request INSTRUCTIONS. Continue health benefits under the SHBP if self-employed or employed by another party during the period of leave.
Please send completed forms below to. Please Submit with the Provider Appeal Form SELECT APPEAL TYPE. Send your completed and signed form to.
Filing Limit Referral Denial Duplicate Claim Corrected Claim Pre-Certification Notification or Prior-Authorization Denials.
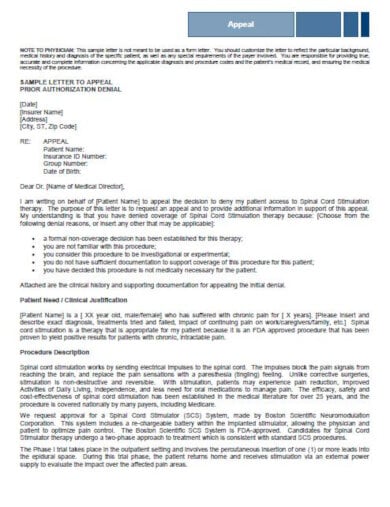
10 Best Medical Appeal Letter Templates Pdf Word Pages Google Docs Free Premium Templates
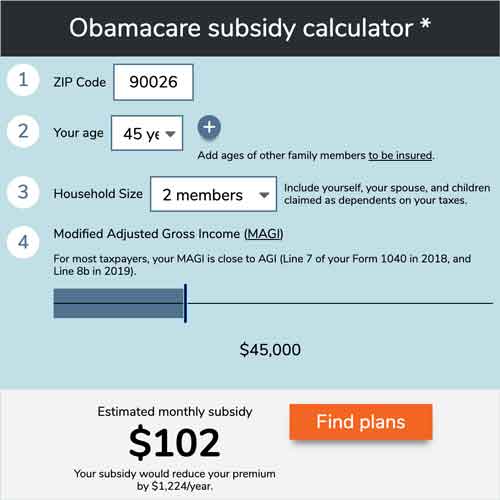
Open Enrollment 2022 Guide Healthinsurance Org

Member Login Healthfirst

Contact Us Mvp Health Care
Surprise Medical Bills New Protections For Consumers Take Effect In 2022 Kff
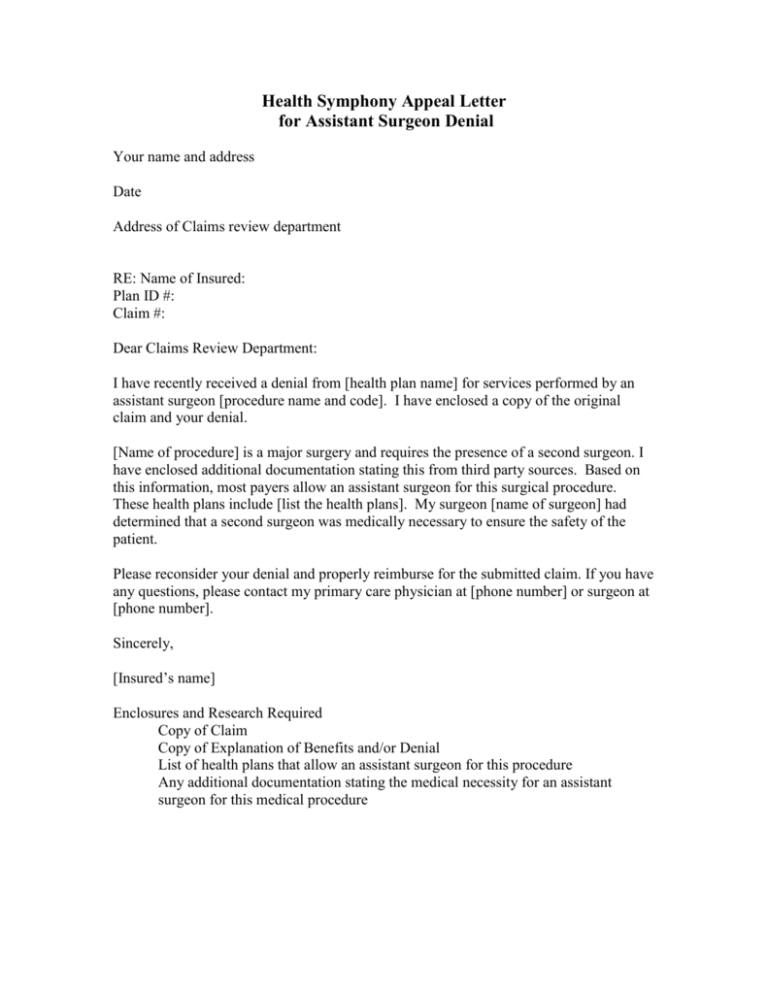
Appeal Letter Assistant Surgeon
Private Health Coverage Of Covid 19 Key Facts And Issues Kff
Https Www Ecommunity Com Sites Default Files Uploads 2016 09 Prohealth Provider Manual Pdf

Health First Colorado Connect For Health Colorado
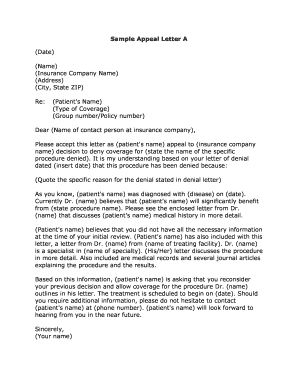
Sample Letter Of Appeal To Health Insurance Company Fill Out And Sign Printable Pdf Template Signnow
Member Login Healthfirst
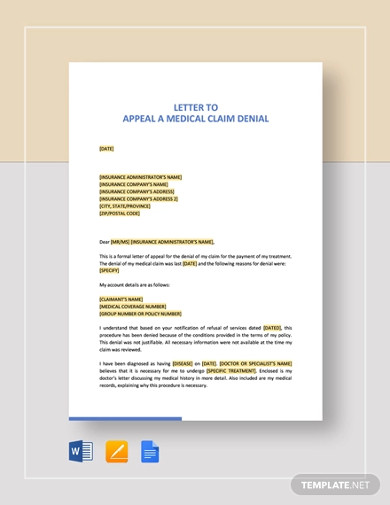
10 Best Medical Appeal Letter Templates Pdf Word Pages Google Docs Free Premium Templates
Https Www Uhcprovider Com Content Dam Provider Docs Public Claims Uhc Single Paper Claim Reconsideration Form Pdf
:max_bytes(150000):strip_icc()/2615505-article-how-to-get-copies-of-your-medical-records-5a74bc258e1b6e0037a24b25.png)
How To Get Copies Of Your Medical Records
10 Best Medical Appeal Letter Templates Pdf Word Pages Google Docs Free Premium Templates
Https Dsiaccesscentral Com Documents 10484001 10482054 Turalio Sample Letter Of Appeal Approved Pdf Ddebbb4c 5336 3704 D2bb 0dff39995b68
10 Best Medical Appeal Letter Templates Pdf Word Pages Google Docs Free Premium Templates
![]()
Community First Health Plans Your Local Health Plan

Community First Health Plans Your Local Health Plan
{kind=link}
Posting Komentar untuk "Health First Health Plans Appeal Form"